





Patrizia Russo, Stefano Bonassi,Robertina Giacconi, Marco Malavolta, Carlo Tomino,Fabrizio Maggi
European Respiratory Journal 2020; DOI: 10.1183/13993003.01116-2020
Nicotine via alpha7-nicotinic receptor induces ACE2 overexpression in Human Bronchial Epithelial Cells (HBEpC)
Leung et al. have recently published in the European Respiratory Journal a paper on the expression of ACE-2 in the small airway epithelia of smokers and COPD Patients, discussing its effects on the risk of severe COVID-19. The authors found an increased expression of the ACE-2 gene in the airways of subjects with COPD and in current smokers. Indeed, a recent systematic review reporting data on thesmoking habit of patients infected with Severe Acute Respiratory Syndrome Coronavirus (SARS CoV)-2, concluded that smoking may be likely associated with a negative progression of the disease and with the adverse outcome. These conclusions were challenged in a correspondence published by Hua Cai on the basis that a reliable mechanism explaining this association was missing.
The need for these results to be supported by additional studies is quite clear, but we believe that a robust mechanistic explanation exists. Nicotine has a known influence on the homeostasis of the renin-angiotensin system (RAS) up-regulating the angiotensin-converting enzyme (ACE)/angiotensin (ANG)-II/ANG II type 1 receptor axis, and down-regulating the compensatory ACE2/ANG-(1–7)/Mas receptor axis, contributing in turn to the development of cardiovascular and pulmonary diseases. Different airway cells, such as bronchial epithelial cells, type II alveolar epithelial cells, and interstitial fibroblasts lung, express nicotinic acetylcholine receptors (nAChR), specifically the α7subtype.
All these cells express components of the RAS. In addition, Nicotine increases the expression and/or activity of ACE in the lung, an increase which have been found also in the serum of smokers, and that required at least 20 min to return to control level. ACE2 serves as a physiologically relevant cellular entry receptor for SARSCoV, for the human respiratory Coronavirus NL63, and probably for the (SARSCoV)-2. The ACE binds the SARS CoV-2 S protein, and through its tissutal expression mediates the localisation and the efficiency of the infection.Moreover, Nicotine induces the epithelial-mesenchymal transition (EMT), a mechanism sufficient to allow “normal” differentiated cells to acquire the stem cell-like characteristics and properties.
We planned experiments on human bronchial epithelial cells (HBEpC), obtained from Cell Applications Inc. (www.cellapplications.com/product no. 502K-05a).Cells were maintained as adherent monolayer in complete bronchial/tracheal epithelial cell growth medium (www.cellapplications.com/product) at 37°C in a 95% air/5% CO2, seeded at an initial density of 7.5×104 cells·cm−2, and sub-cultured with a 0.25% trypsin–1 mM EDTA solution (Sigma-Aldrich, Milan, Italy) when cultures reached 80% confluence. HBEpC are derived from the surface epithelium of normal human bronchi non-diseased (i.e. Asthma, COPD, or Type 2 Diabetes).
The morphology is consistent with epithelial origin, and is positive for epithelial cell marker cytokeratin 18. Semi-confluent HBEpC at 4th passage (7.5×104 cells·cm−2) were treated:(a) for 1 h with zero or 1.0×10−7 M Nicotine (Sigma–Aldrich, Milan, Italy) dissolved in saline in complete medium; (b) with 1.0×10−6 M α-Bungarotoxin (α-BTX, Sigma–Aldrich, Milan, Italy)dissolved in saline, in the continued presence of nicotine at zero or 1.0×10−7 M for 1 h; (c) treated continuously with nicotine for additional passages, 1 passage every 48 h for a total of 16 passages.
We showed, for the first time, that nicotine at 1×10−7 M (the concentration present on the alveolar lining fluids after one cigarette is in the range 6×10−6 to 6×10−5 M is able to increase ACE2 in HBEpC. Treatment with nicotine induces phospho-S6 ribosomal protein (Ser235/236), Akt1, phospho-Akt (Ser473), phospho-Akt(Thr308) and phospho-p44/42 MAPK (Thr202/Tyr204) .To verify the hypothesis that ACE2 is induced by nicotine through α7-nAChR, HBEpC, at 4th passage, in the exponential growth phase, plated at a density of 1×106 cells·mL−1, were incubated with α7-nAChR siRNA (0.1 μg) diluted in 100 μL of siRNA transfection medium.
Transfection was performed as described by Li et al., who transfected, successfully, HBE16 human airway epithelial cell line (unaffected cells).A clone of transfected HBEpC that did not express α7-nAChR proteins, also after treatment with nicotine, and is not able to induce phospho-S6 ribosomal protein (Ser235/236), Akt1, phospho-Akt (Ser473), phospho-Akt(Thr308) and phospho-p44/42 MAPK (Thr202/Tyr204) after nicotine treatment, was selected for further experiments. Nicotine did not induce ACE2 in this clone (si-mRNA-α7-HBEpC).
This observation supports the hypothesis that ACE2 increase is specifically mediated by α7-nAChR. Moreover, when HBEpC were incubated simultaneously with nicotine and α-BTX, an α7 nicotine antagonist, no induction of ACE2 was observed . Importantly, treatment with Nicotine, α-BTX or with the combination is not cytotoxic (data not shown).On these bases, we suggest that smoking may promote cellular uptake mechanisms of SARS CoV-2 through α7-nAChR signalling.A possible α7-nAChR down-stream mechanism may be the induction of phospho-Akt and phospho-p44/42 MAPK. This mechanism was hypothesised, partially, by Olds and Kabbani on their schematic model explaining how nicotine exposure increases the risk of COVID-19 entry into lung cells. α7-nAChRis present both in neuronal and non-neuronal cells (i.e. lung, endothelial, lymphocyte) consequently smoking may impact COVID-19 pathophysiology and clinical outcome in several organ systems including brain.

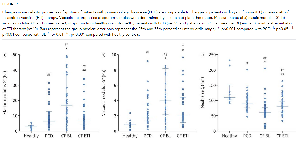
Effect of nicotine on HBEpC or si-mRNA-α7-HBEpC. Panel a) ACE2 detection. ACE2 was measured with Human ACE2 ELISA Kit ab235649 (www.abcam.com/human-ace2-elisa-kit-ab235649.html) according to manufacture instructions. Data are mean±se; p was evaluated using t-test. The green plots are the human ACE2 standard. Experiments were performed twice in triplicate. Panel b) Induction of phospho-S6 ribosomal protein (Ser235/236), Akt1, phospho-Akt (Ser473), phospho-Akt(Thr308) and phospho-p44/42 MAPK (Thr202/Tyr204) in HBEpC. Data were obtained using PathScan® cell growth Multi-target Sandwich ELISA kit n.7239 (Cell signalling) PathScan® Cell Growth Multi-Target Sandwich ELISA Kit is a solid phase sandwich enzyme linked immunosorbent assay (ELISA) that combines the reagents necessary to detect endogenous levels of S6 ribosomal protein, phospho-S6 ribosomal protein (Ser235/236), Akt1, phospho-Akt (Ser473), phospho-Akt(Thr308) and phospho-p44/42 MAPK (Thr202/Tyr204).Data are mean±se; p was evaluated using t-test. Experiments were performed twice in duplicate. Panel c) α7-nAChR protein detection. Western Blotting was performed as described previously . Human α7-nAchR antibody NBP1-49348 was purchased by Novus Biologicals [www.novusbio.com]. 1–2 si-mRNA-α7-HBEpC treated with zero (lane 1) or 1.0×10−7 M Nicotine (lane 2) for 1 h. 3–4 HBEpC treated with zero (lane 3) or 1.0×10−7 M Nicotine (lane 4) for 1 h. Experiments were performed twice. Panel d) as in Panel (b), treated cells are si-mRNA-α7-HBEpC.
Footnotes
-
Conflict of interest: None to discose
-
Conflict of interest: None to disclose
-
Conflict of interest: None to disclose
-
Conflict of interest: None to disclose
-
Conflict of interest: None to disclose
-
Conflict of interest: None to disclose
- Received April 10, 2020.
- Accepted April 16, 2020.
- Copyright ©ERS 2020







{kind=link}