





Diffusing capacity of the lung for carbon monoxide (DLCO) reflects the capacity of carbon monoxide (CO) transfer from the environment to the pulmonary capillary blood, which is the most clinically useful routine methodology to evaluate the function of the lung to exchange gas. KCO is the rate constant for CO uptake from alveolar gas, which is influenced mostly by the thickness and area of the alveolar capillary membrane, the volume of blood in capillaries supplying ventilated alveoli, and the concentration and properties of hemoglobin (Hb) in the alveolar capillaries blood. DLCO is mainly determined by KCO and the alveolar volume (VA). Mathematically, KCO can be calculated as DLCO/VA under body temperature, ambient pressure, saturated with water vapor (BTPS) conditions.
We agree with Dr. Nusair that it should be noted that DLCO/VA is not a simple ratio and in fact the relationship between lung volume and CO uptake is linearly and certainly less than 1:1 . Recent studies have tended to use KCO instead of DLCO/VA, as DLCO/VA may be inferred that DLCO can be normalised for VA. The 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung recommends that the term of KCO is better way than DLCO/VA . However, in practice, many pulmonary function test reports from different manufacturers still present with DLCO/VA but not KCO. Besides, in order for an easier and direct comparison with some previous studies on pulmonary function in patients with SARS , DLCO/VA was kept in our report. It is important to understand the interpretation of KCO and DLCO/VA, the term of KCO is recommended for more popular use in future.
Decreased KCO occurs in alveolar-capillary damage, microvascular pathology, or anemia. Causes of low VA includes reduced alveolar expansion, alveolar damage or loss, or inspired gases maldistributed with airflow obstruction. When KCO turns normal, in the presence of a low DLCO it is associated with low VA. Because only the functional alveolar unities had been sampled thereby providing a biased picture toward more preserved areas of the lungs . Crucially, the same DLCO may occur with various combinations of KCO and VA, each suggesting different pathologies. It is difficult to interpret which is the predominant role because both decreased alveolar volume and KCO contribute to the pathogenesis of impaired diffusion capacity. DLCO gives an overall assessment of gas exchange for the lung, while the alveolar-capillary membrane diffusing capacity for carbon monoxide (DMCO) only dependents on molecular diffusion of the membranes. However, DMCO can be calculated using different equations but not unified yet, which is not a commonly used gas diffusing parameter .
In our study, 51 patients with COVID-19 had impaired DLCO, including 29 patients who showed both impaired DLCO and KCO. The number of patients with both impaired DLCO and KCO (29/51) was 24% bigger than the number of patients with impaired KCO alone (22/51). Moreover, the percentage of patients with decreased TLC was less than the percentage of patients with decreased KCO. Furthermore, vascular injury and thrombosis are demonstrated important contributing factors in the pathogenesis of COVID-19. SARS-Cov-2 infects the endothelial cells by angiotensin converting enzyme 2. The recruitment of immune cells to the endothelial cells facilitates the induction of endotheliitis in several organs which contributes to the systemic impaired microcirculatory function . Acute pulmonary embolism has been reported during the clinical course . Postmortem studies reported the vascular injury and thrombi in multiple organs . Ackermann et al. compared the lung pathology of COVID-19 with H1N1. The result showed that patient with COVID-19 presented distinctive vascular features, consisting of severe endothelial injury associated with the disruption of intercellular junctions, cell swelling and a loss of contact with the basal membrane. From the above, it is considerable that the effect of membrane lesion plays an important role on the impaired diffusion capacity in patients with COVID-19.
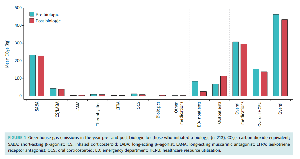
Our study showed that, similar as DLCO, DLCO/VA (represents the transfer factor of carbon monoxide) also showed an association with the disease severity: As the patients underwent more severe condition, mean value of DLCO/VA of predicted was lower. Since standard deviation value suggest that individual differences have effects on lung function, we had also provided the distribution of the DLCO/VA of predicted in patients with different severity. 42% of the subjects with severe pneumonia had a DLCO/VA of predicted less than 80%, while only 27% in the patients with pneumonia and 13% in patients with mild illness, respectively.
In previous follow-up studies of SARS, the impaired DLCO was defined as when DLCO was <80% of the predicted value irrespective of the KCO or the alveolar volume. In the follow-up studies of rehabilitating SARS patients ranging from 0.5 to 2 years, the impaired DLCO was the most common abnormality, accounting for 15.5% to 43.6% . The mean of the DLCO/pred% ranged from 77.7% to 93.8% in the studies above with the longest follow up of 2 years. Our study showed a mean of DLCO/pred% for 78.2% at time of discharge but the data of follow up is not available yet. It is unclear how the impaired diffusion capacity change in survivors of COVID-19, as well as in the chest CT. In one study, where surviving SARS patients were seen 6 months after admission, 43(75.4%) of patients showed radiological abnormalities, including 62.8% had abnormal DLCO . Thus, the lung function impairment findings are consistent with the CT images of SARS survivors showing persistent ground glass opacity, reticular opacities and traction bronchiectasis suggesting the fibrosis. Likewise, in discharged patients with COVID-19, Wang et al. reported that 94% (66/70) of patients who were discharged from hospital at the end of the study still had mild to substantial residual lung abnormalities on their last CT scans .
Our study was a pilot study which firstly described the impaired pulmonary function in patients with COVID-19 at time of discharge. Impairment of diffusion capacity is the most common abnormality followed by restrictive ventilatory defects. However, more work ahead for follow-up is needed to assess the longitudinal variation of these deficits.
Footnotes
-
Conflict of interest: Dr. Chen has nothing to disclose.
-
Conflict of interest: Dr. Gao has nothing to disclose.
-
Conflict of interest: Dr. Chen has nothing to disclose.
-
Conflict of interest: Dr. Jian has nothing to disclose.
-
Conflict of interest: Dr. Lei has nothing to disclose.
-
Conflict of interest: Dr. Zheng has nothing to disclose.
-
Conflict of interest: Dr. Li has nothing to disclose.
- Received June 6, 2020.
- Accepted June 11, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.








{kind=link}