Abstract
Pulmonary arterial hypertension (PAH) is a rare form of precapillary pulmonary hypertension. PAH may be idiopathic, heritable, associated, with features of pulmonary veno-occlusive disease and/or pulmonary capillary hemangiomatosis, or linked to drug and toxin exposure. Since the first identification of PAH cases associated with drugs and toxins more than 50 years ago, the number of suspected agents has significantly increased. Since the 6th World Symposium drugs and toxins are classified as definitely or possibly associated with PAH: there are currently 9 drugs considered as definitely associated with PAH, and 16 considered as possibly associated with PAH. In the 7th world symposium on pulmonary hypertension carfilzomib and mitomycin C were added as definitely associated with PAH, while bevacizumab and bortezomib were considered as possibly associated with PAH.
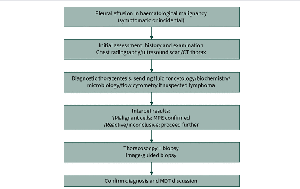
In cases of suspected PAH following drug or toxin exposure, specific measures are required, including pharmacovigilance reporting, echocardiography, right heart catheterization to confirm the diagnosis, and potential initiation of targeted treatment. Here, we review the latest updates on PAH associated with drugs and toxins.
This is a PDF-only article. Please click on the PDF link above to read it.
Footnotes
This manuscript has recently been accepted for publication in the ERJ Open Research. It is published here in its accepted form prior to copyediting and typesetting by our production team. After these production processes are complete and the authors have approved the resulting proofs, the article will move to the latest issue of the ERJOR online. Please open or download the PDF to view this article.
Conflict of interest: Jason Weatherald reports grants from Janssen, 35Pharma, Merck, Astra Zeneca, Sanofi; Consultancy fees from Janssen, Merck, Apollo Therapeutics; Payment or honoraria for lectures, presentations, manuscript writing or educational events from Janssen, Merck, United Therapeutics; Payment for expert testimony from Sprigings Intellectual Property Law; Support for attending meetings from Janssen, Merck; Participation on a data safety monitoring board or advisory board with Janssen, Merck, Université Laval, Cambridge University; Leadership role with Pulmonary Hypertension Association of Canada, Pulmonary Vascular Research Institute.
Conflict of interest: Montani David reports grants from Acceleron, Janssen, Merck MSD; Consultancy fees from Acceleron, Merck MSD, Janssen, Ferrer; Payment or honoraria for lectures, presentations, manuscript writing or educational events from Bayer, Janssen, Boehringer, Chiesi, GSK, Ferrer, Merck MSD; Currently serving on the ERJ Open Research editorial board as an Associate Editor.
Conflict of interest: Marc HUMBERT reports grants from Gossamer, Merck; Consultancy fees from 35 Pharma, AOP Orphan, Chiesi, Ferrer, Gossamer, Janssen, Keros, Liquidia, Merck, Novartis, Regeneron, Respira, Roivant, United Therapeutics; Payment or honoraria for lectures, presentations, manuscript writing or educational events from Merck; Participation on a data safety monitoring board or advisory board with 35 Pharma, Janssen, Keros, Merck, Novartis, United Therapeutics.
Conflict of interest: Laurent SAVALE reports grants from Acceleron, AOP Orphan, Janssen, Merck, Shou Ti; Consultancy fees from Acceleron, Bayer, Janssen, Merck; Payment or honoraria for lectures, presentations, manuscript writing or educational events from Janssen, Merck.